international symposium on leprosy |

|

Day 2: Tuesday January 24, 2023 (Augustinianum Patristic Institute, Rome)
Leave No One Behind
Leave No One Behind
Theme: Toward Realizing a Society in Which No One Is Left Behind
Keynote speech: What has been the impact of the Covid-19 pandemic on the socially vulnerable, especially those who have disabilities? Dr P Narasimha Rao, President, International Leprosy Association and Indian Association of Leprologists

Dr P Narasimha Rao
Dr Rao said that those with disability found it harder to access critical supplies and medical support during the pandemic. He argued that combining physical with virtual services could be harnessed in the future. He added, that when Covid-19 is controlled, there will be lessons and technology developments that can be used.
|
Missed disability in those examined for leprosy
Leprosy reaction due to Covid-19 or the vaccine
More Grade 2 Disability among new cases of leprosy
|
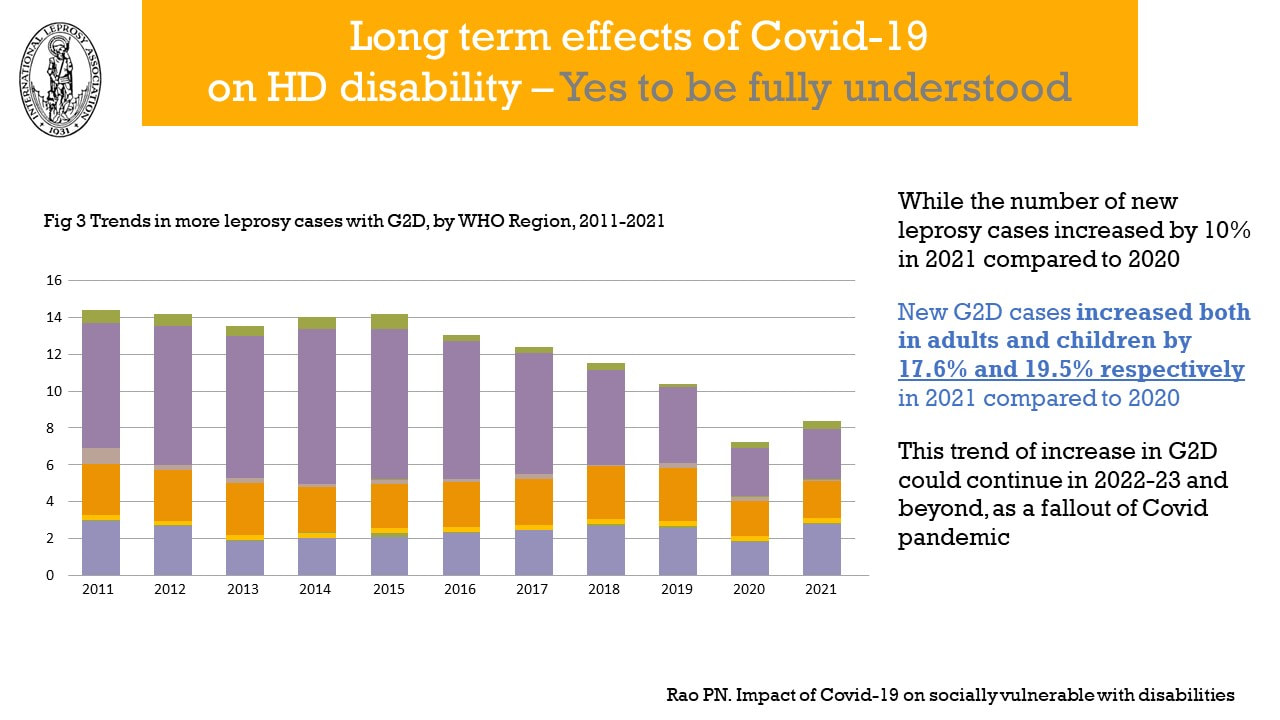
Long-term effects of Covid-19 on leprosy disability

New measures to reduce the impact on healthcare
|
Testimony (Moderator: Mr Amar Timalsina, Executive Director, IDEA Nepal)

Amar Timalsina
At the start of the session, a video was shown to delegates. It told the distressing and tragic story of Ms Dimby and her daughter, nine-year old Ms Soavina (with leprosy reaction) both affected by leprosy, living in Madagascar.
Ms Dimby and Ms Soavina were treated at the Marana Leprosy Centre.
|
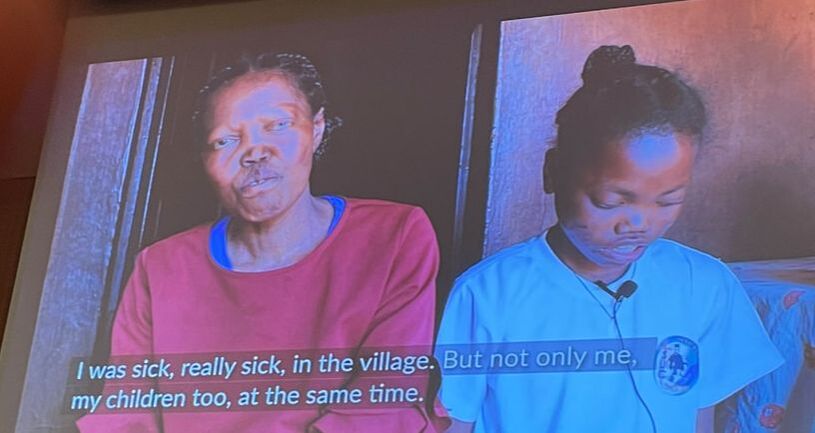
I was sick, really sick, but not only me. My children too at the same time.
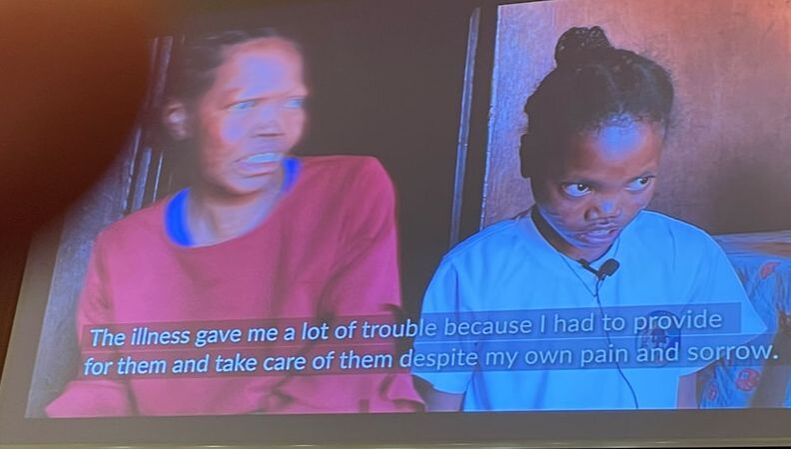
The illness gave me a lot of trouble because I had to provide for them and take care of them despite my own pain and sorrow.
SFLG supports the Marana Centre, Madagascar.
|

Rajni Kant Singh, State Coordinator for Bihar Operations, LEPRA Society, India
Mr Rajni Kant Singh spoke by video from Bihar. He works there for Lepra and is a person affected by leprosy. He said:
we must manage leprosy reaction(s) to prevent disabilities. People affected by leprosy in remote locations could be empowered to collect data. |
|

Patricia Goncalves Soares, Coordinator, Department of Policies for Women, Morhan, Brazil
Ms Goncalves Soares said that there were many challenges faced by people affected by leprosy in Brazil, similar to those experienced by people from other countries. She thought that collective strategies for a better quality of life for people affected were needed. Holistic treatment was also needed to enable people with leprosy to live with dignity and not be seen as statistics or a disease. People affected by leprosy wanted their voices heard. She said that the only way to achieve solutions was to hear about the problems. She added that we shouldn't be ashamed of a curable disease but should have access to quality care and humane and respectful treatment. She called for doctors and healthcare operators to join forces and help people affected on their journey. She said:
|

We have a disease, but that doesn't mean we can't live full lives. We don't want to be considered disabled. Although leprosy is a neglected disease, we should make sure that people affected by leprosy are not neglected or ignored. We must make sure that our rights are respected everywhere. We all face challenges, but we all want to be respected and to live a dignified life; not the life that others might expect for us. We should not be defined by our disease. I urge delegates to speak up on our behalf."
Best Practices with special attention to the roles of religious organizations (Moderator: Patrice Simmonet, Director General, AIFO)

Patrice Simonnet
Mr Simonnet said he wanted to thank everyone who worked in the field - whose faces we don't often see.
Mr Thierry zen Ruffinen, President, Fondation CIOMAL de l'Ordre Malte.
Mr zen Ruffinen referred to the Order's First Rule (Matthew chapter 25, verse 40), its 924 year history starting in 1066 and the leprosaria it ran throughout Europe. He mentioned Cambodia's tragic history with high levels of leprosy and CIOMAL being tasked to run its national leprosy programme. He proposed that leprosy was a problem for all of society because it was a disease that scared us all.
CIOMAL's First Rule - Matthew Chapter 25 verse 40
Selected Chapters of CIOMAL's Living History
|
Sr Sabine Ramasinoro, Head of Marana leprosy centre, Madagascar
Sr Sabine said that anyone who arrived at the Marana centre was screened for leprosy. Former patients were good at tracking down and identifying people suspected of leprosy and then encouraging them to get treated at the centre.
Sometimes people with leprosy arrived at the centre asking for clothes and provisions. The sisters recognised these people as human beings and washed, clothed and fed them, before treating them for leprosy. When a leprosy diagnosis was confirmed, the centre provided food, treatment and shelter. People with leprosy could stay until they were completely healed or, as long as they needed. A skin patch was all that was required for an invitation to stay or return for treatment. There were currently 110 people affected by leprosy living at the centre. Some were new patients, some longer-term patients and some lived there because they could not return home.
The centre provides physical rehabilitation, performs surgery (including for nerves), amputations, and skin treatment. They have an education and training centre, so that people can learn new skills and make a living. There is secondary education for younger patients and vocational training too. Sr Sabine mentioned that there is a shoe shop nearby owned by a former patient, who was only too happy to help with their shoes. Their gardener produces fruit and vegetables. There was cooperation with the local diocese to allow former patients to work with wood and timber in local construction. The centre was one big happy family. Patients helped to keep the centre clean and tidy and everyone had their own duties. St Francis Leprosy Guild supports the Marana centre, Madagascar.
|
Dr Jose Manikkathan, Director AIFO, India
Dr Jose Manikkathan said there are many challenges to overcome in the north-east Indian states and some organisations would not even consider this location as (operationally) viable. The capacity to diagnose leprosy is almost nil, so terrible deformities arise and many people live with the consequences, and at a severity not encountered elsewhere. He said that there are around 800 tea plantations in Assam with workers from other Indian states, with many cases of undiagnosed leprosy. Many people need treatment for leprosy reaction too. He knows of a family where eight out of nine children are affected by leprosy.
He concluded that they needed a new cadre of leprosy worker in this location, with a collective effort to pool resources and ensure early diagnosis. He said: Every case of Hansen's is one case too many." 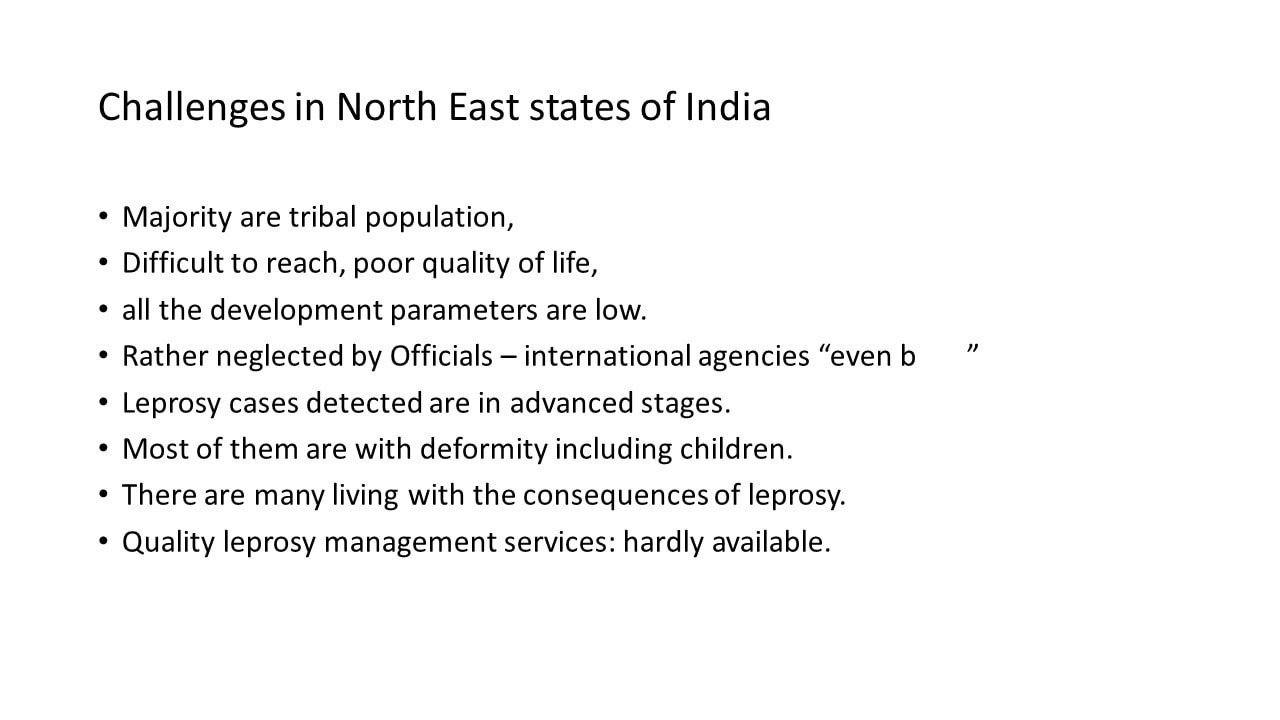
Challenges in the north-east Indian states.
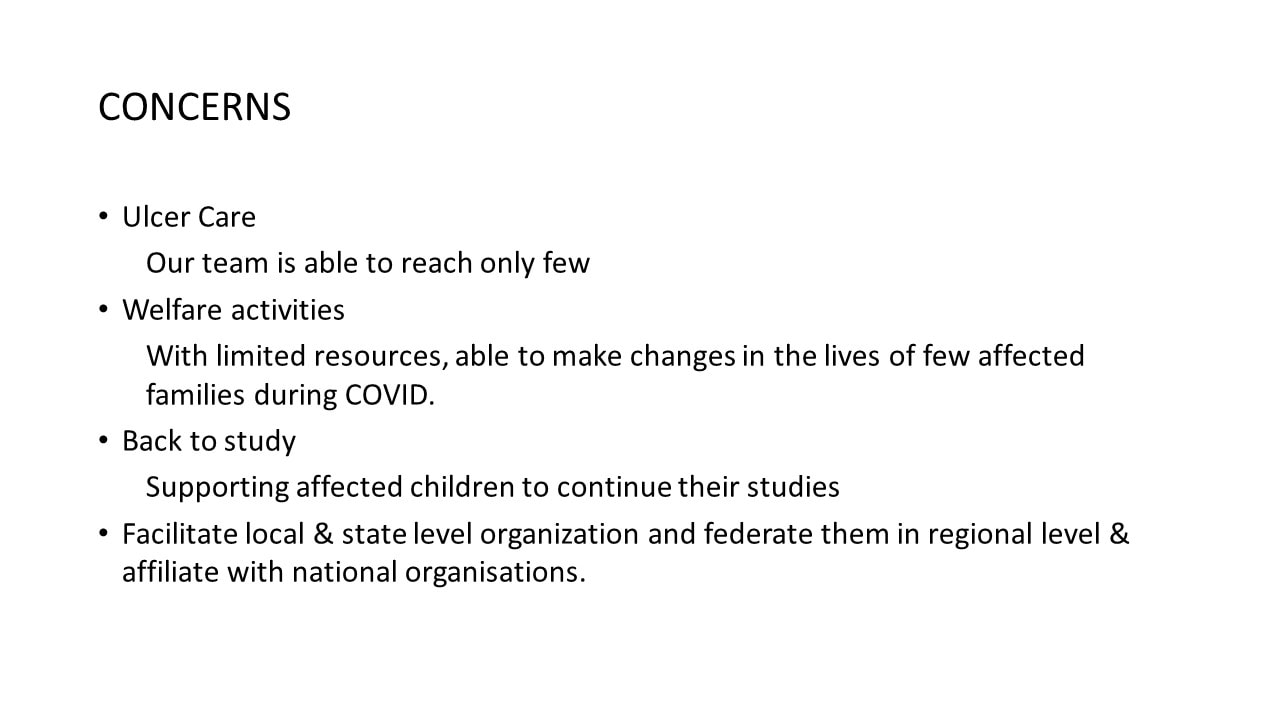
Concerns

A girl with severe lepromatous leprosy
|

Sr Mary Bawani Chelliah, Order of Franciscan Missionaries of Mary, Sri Lanka
Sr Bawani presented the work of the Franciscan Missionaries of Mary (FMM) in Sri Lanka during the Covid-19 pandemic.
Sr Bawani currently lives at the FMM convent in Rome but for twenty years she worked at the Manthivu leprosy hospital in Sri Lanka. After the hospital's repatriation by the Sri Lankan government in 1964, the FMM Sisters sought and were granted permission to continue their hospital visits and community outreach work. A summary of their outreach activities is shown below: Summary of outreach activities
Summary of further outreach activities
Much of the Sisters' work involves long, uncomfortable travel to remote locations where people with leprosy often live. The Sisters act as confidente and "treat as a friend" all the people affected that they visit.
During the pandemic, although there were travel restrictions, the Sisters continued their outreach unabated. Much of the work entailed the provision of food, rations and medication. The people affected were mostly elderly, isolated and extremely poor. There was little or no provision for people affected by leprosy during the pandemic and it is likely the Sisters saved many lives. See Sr Bawani's full presentation Watch the video |

Sr Gladis Estela Llano Uribe, Director of Villa Bernarda Foundation, Colombia
Sr Gladis spoke about the need for social inclusion for people with leprosy, improving the quality of their life, empowerment and the elimination of stigma, all of which remain challenges. At Villa Bernarda Foundation, they arranged workshops, health visits, support for people with disabilities and education of young people, all aimed at the re-integration of people with leprosy. She said:
When we are alone we are invisible. When we are united, we are invincible." Questions were invited from the floor.
All panellists concurred that early leprosy diagnosis was critical to prevent leprosy disability and stigma. Sr Bawani thought that self-awareness was important for all people with leprosy so they can say. "If I know I have leprosy, I can get treated." |

Sr Gladis Estella Llano Uribe, Sr Sabine Ramasinoro, Sr Mary Bawani Chelliah
Recommendations and suggestions on how to move forward from the conclusions and recommendations adopted in 2016 (Moderator: Msgr Robert J Vitillo, Secretary General, International Catholic Migration Commission)
Session 1: Perspectives of key actors from the Global Leprosy Community

Dr Vivek Lal, Team Leader, Global Leprosy Programme, WHO

Dr Alice Cruz, UN Special Rapporteur on the elimination of discrimination against persons affected by leprosy and their family members
Dr Cruz said by video link that Covid-19 had disrupted leprosy healthcare. She added that the world had also changed with a terrible war and global warming which have a greater effect on the countries of the global south. We needed to work out their impact or the lack of impact. We need follow-up mechanisms with people on the ground and organisations working at the national and local level. Our vulnerable communities are more vulnerable than ever before. She asked:
How do we engage with these "big issues" - climate change and extreme poverty, that block access to treatment and the elimination of discrimination." |

Dr Margarida Cristiana Napoleao Rocha, Technologist, Ministry of Health, Brazil
Dr Rocha said that Brazil's national leprosy strategy was developed with persons affected by leprosy. She believed that a common, collective document could lead to empowerment.
This outlook meant the early discovery and treatment of leprosy and an integral approach with five cross-cutting elements: stigma and discrimination, scientific research, access to communications, access to monitoring epidemiology and an IT system. Empowerment, early diagnosis and treatment and integration into society lead to psychosocial recovery. |

Dr Benedict Quao, National Programme Manager, National Leprosy Control Program, Ghana
Dr Quao said it was clear that considerable progress had been made in the fight against leprosy, but it was clear too that there was still a lot to do. However, it was very encouraging for countries to see such committed actors and to know that there are partners to help.
We need a unified approach and to form national partnerships and roadmaps. People affected by leprosy want a voice. In Ghana people affected are involved with the design of programs and maintaining the quality of the programs. We get so bogged down with data, when everything we do should be person-centered and about the quality of service. Empowering people affected by leprosy means they can fight for their rights. |

Geoff Warne, CEO ILEP
Mr Warne said from the ILEP perspective, their view from 2016 was that every case of leprosy was one case too many.
The WHO GLS 2021-2030 is all about reduction and challenging targets which may be achievable with current and new tools. ILEP members work with governments to implement the strategy and scale up. The elimination of stigma and discrimination is more challenging and we have to urge governments to support this goal. Self-help groups are known to help with fighting exclusion. |

Bill Simmons, CEO, American Leprosy Missions, Chair Global Partnership for Zero Leprosy
Mr Simmons said that countries have demonstrated their co-operation to work together and we have heard from people affected by leprosy.
Then he read out Luke chapter 17, verse 11, Jesus Heals Ten Men with Leprosy. He said that he took his inspiration from Jesus' approach and how we should approach zero leprosy. Jesus brought them access to healthcare. He brought healing to them and He sent them to the priests (to be re-included into society). Jesus demonstrates, in this 2000 year-old example, what it means to Leave No One Behind. He read as follows: |

Dr P Narasimha Rao, President, International Leprosy Association and Indian Association of Leprologists
Dr Rao said that he concurred with the 2016 statement that every case of leprosy was one case too many. He said that there is a need for more scientific research in relation to early diagnosis and the management and prevention of complications and disability. There is an explosion of new cases in India and many parts of the world and many are becoming multibacillary cases; 55% MB cases up from 30%. Without more research and active case-finding for early diagnosis, we cannot prevent stigma.
|
"11 Now on his way to Jerusalem, Jesus traveled along the border between Samaria and Galilee. 12 As he was going into a village, ten men who had leprosy met him. They stood at a distance 13 and called out in a loud voice, “Jesus, Master, have pity on us!” 14 When he saw them, he said, “Go, show yourselves to the priests.” And as they went, they were cleansed. 15 One of them, when he saw he was healed, came back, praising God in a loud voice. 16 He threw himself at Jesus’ feet and thanked him—and he was a Samaritan. 17 Jesus asked, “Were not all ten cleansed? Where are the other nine? 18 Has no one returned to give praise to God except this foreigner?” 19 Then he said to him, “Rise and go; your faith has made you well."" Luke chapter 17, verse 11

Arielle Cavaliero, Global Business Director, Leprosy Global Health Program, Novartis
Ms Cavaliero said that she was looking at leprosy with a fresh pair of eyes, as she had not attended the 2016 symposium. She had agreed with many comments.
She felt encouraged that ILEP, GPZL and the WHO GLS have all made similar recommendations. She said: we are clear what needs to happen but how do we get there? Who are the targets and agents of change (and expertise)? What is the ask? What are the targets we want to set? We need monitoring to understand our success. We need to consider the barriers that prevent us from learning. She said the recommendations and strategies are powerful. How do our ambitions harmonise? We must continually explore how people affected by leprosy can be empowered to be the drivers for change. |

Letitia Cezar da Frota, Miss World Brazil 2022
Ms Frota said that a Beauty Queen without a cause was worthless. She said that wherever she goes she tells people about Hansen's Disease; that it is a real disease and closer than we can imagine.
She added, if she can use her crown to give a voice to those who need it, why not? She has visited people affected by leprosy in the Amazon to find out their needs. The children are the best channel to reach their parents and relatives. She said she has also visited India and with Miss World India they will get the message out to the world. Together we are much stronger. She said that she dreams that we will reach the zero leprosy target. |
Maya Ranavare, President, Association of People Affected by Leprosy (APAL) India and representative of the 2nd Global Forum of People's Organizations on Hansen's Disease (Gaurab Sen translating)
Ms Ranavare said it was her suggestion that people affected by leprosy should be part of all processes and not just the beneficiaries. This point was discussed at the ILC in Manila 2019 and in Hyderabad 2022. She urged/recommended that there should be a follow-up committee from all countries to ensure progress. She asked if there should be a letter signed by all countries. It is not enough to have recommendations - they need to be put into practice. We need to put pressure on all governments (and not just those related to ILEP members) so that our goals get put into government structures. She re-emphasised:
Nothing About Us Without Us." |
Session 2: Perspectives of the Organizers

Patrice Simonnet, Director General AIFO
Mr Simonnet said we will continue the fight for equality and against poverty.
The Global Appeal 2023 contains a very important message "Don't forget people with leprosy," so we must communicate better, keep working together, recruit more volunteers, keep networking (for example ILEP and GPZL), hire qualified staff who understand the challenges, engage in international cooperation, explain better, combat war and legal restrictions and deal with the shortage of skilled staff. We must identify new resources and organise a world that is different. |

Mr Oleg Ouss, Chairman, Raoul Follereau Foundation
Mr Ouss thanked everyone affected by leprosy who had shared their experiences.
He believes that a holistic approach is important. We must take advantage of our strengths to deal with "the last mile" in the fight against leprosy and allow everyone involved in the struggle to participate. Dignity and respect have been mentioned often at this meeting as have education and self-esteem, and a meaningful life - the spiritual dimension of human beings. Pope Francis' message was important and other religious leaders can follow his example. On a public and private level, being isolated can lead to a loss of resources. For example, some countries have little government involvement. We must work with former patients and it was disappointing that people with leprosy have been refused visas for this conference. He said: Through our rage we must show love. People affected by leprosy, please help us to put love into everything we do. Without love nothing is possible but with love, everything is possible." |

Dr Takahiro Nanri, Executive Director, Sasakawa Health Foundation/Sasakawa Leprosy Initiative
Dr Nanri said we need a concrete commitment on how we respond to the five recommendations.
Zero leprosy means realising a world free from disease, fear and discrimination. To tackle disease we will work with the WHO, GPZL and ILEP, target governments, support research (to develop new tools to prevent and treat leprosy) and maximise the influence of the Goodwill Ambassador. To eliminate discrimination we will implement the Principles and Guidelines and seek the modification or abolition of all discriminatory laws. We will research and investigate the current state of stigma and discrimination suffered by people affected by leprosy as evidence to target governments. We will keep advocating to the international community. We will preserve history to promote transformation and enhance leprosy services. We will build a museum in Japan and create archives. We will raise awareness that leprosy is curable and there is no need to discriminate. We will develop unified and joint plans and develop cooperation. We will organise the 21/22 June meeting in Bergen which will include more scientific aspects. This year, we will commemorate the 150th anniversary of the discovery by Dr Armauer Hansen in 1873, of the bacterium that causes leprosy. |

Msgr Robert J Vitillo
|
I have heard about the importance of partnerships in research, of political commitment, of guidelines, of action against discriminatory laws, of awareness-raising throughout all of society and involving religious leaders to engage congregations. Now go out and put all of this into practice! If you want peace, work for justice." |
Wrap-up & Closing Remarks
Msgr Charles Namugera, Dicastery for Promoting Integral Human Development, Holy See
Msgr Charles Namugera, Dicastery for Promoting Integral Human Development, Holy See

Msgr Charles Namugera
|
I have listened to many speakers and on many approaches relating to the end of leprosy and, especially, empowering people with leprosy to become agents of change. Pope Francis said yesterday that we must ask ourselves, how best to work with people with leprosy to live as full members of our community." |
Delegates were invited to attend an audience with His Holiness Pope Francis on Wednesday 25 January 2023.
His Holiness welcomed the delegation during his address.
Leave No One Behind
|
|

|
|

